Updated Every Month
March 1st marks one year since COVID-19 vaccines were first distributed by an African country. Since then, African countries have only been able to procure 633 million vaccines with over 60% of these doses already administered. To bring this into focus, just one country – the US – with a population a quarter the size of the African continent, has administered over 550 million vaccines over the same period, and procured a great deal more. While this overall disparity in vaccine access is highly problematic for countries attempting to control the spread of COVID-19, the type of vaccine procured is also important, and our data this week reveals some very distinct – and worrisome – patterns when it comes to African countries, especially in terms of the ability to manage COVID-19 in future.
This month, our data reveals that the most popular COVID-19 vaccine across African countries is the viral vector J&J vaccine – representing 25% of African vaccine procurement. The pros: It requires minimal infrastructure for distribution and has a single dose schedule and therefore is easy to distribute widely. However, there are some cons. This vaccine in particular has been associated with the rare occurrence of blood clots following vaccination. Whilst this poses a small health risk to individuals, reports such as these have a negative impact on vaccine uptake. The need to tackle this vaccine hesitancy and reassure the public is therefore heightened for many African governments.
Furthermore, treatment of the rare conditions associated with the J&J vaccine is available – however, to be effective these treatments require health infrastructure that provides fast and accurate diagnosis… Infrastructure that is not always available across the continent.
Evidence is also growing in favour of using “heterologous” approaches for COVID-19 immunization – i.e. the use of multiple vaccine types – and has been used to tackle a number of other viruses and diseases. In the context of COVID-19, the use of viral vector vaccines (like J&J) and mRNA vaccines (like Moderna) in combination have shown to have an improved immune response, especially when an mRNA vaccine is used as a booster.
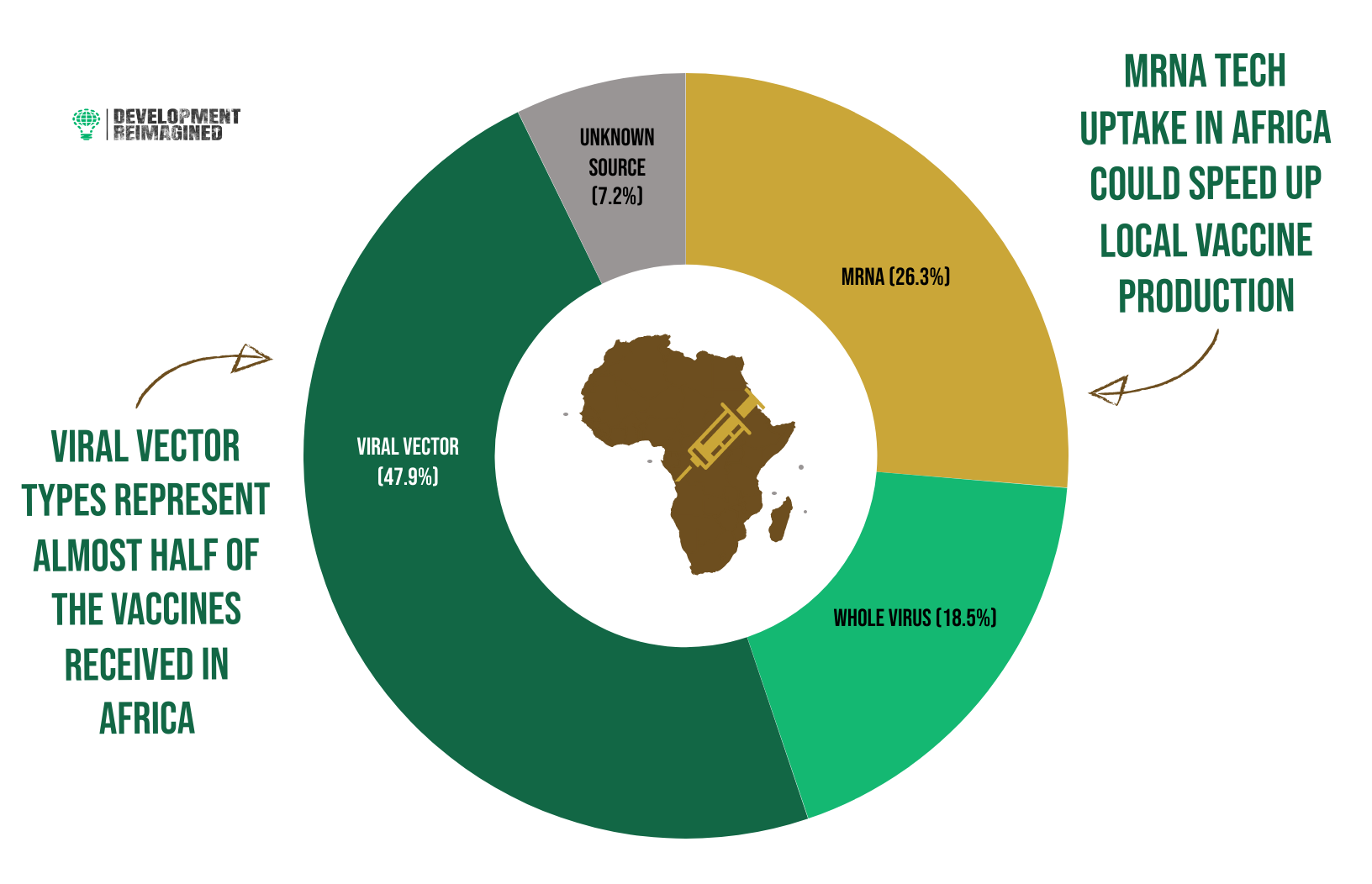
Yet, so far, less than 3% of vaccines administered on the African continent have been boosters. Furthermore, only 26% of vaccines procured in African countries are mRNA vaccines, with Pfizer representing 19% of the vaccines procured and Moderna only 7%. Vector vaccines as a whole represent 48%. If a heterologous approach is more effective to prevent the spread of COVID-19, African governments will need to focus on procuring more mRNA vaccines.
But here’s the rub again. mRNA vaccines require specific and technical infrastructure investment both for their production and their distribution. Currently, there is only one site across the continent that has the infrastructure to produce mRNA vaccines! Whilst African governments are looking to change this – for example Egypt, Kenya, Nigeria, Senegal, Tunisia And South Africa have all committed to investing in WHO tech hubs for local MRNA production – this change needs to happen quickly. As we have set out in previous reports, it also requires structural change not only to African pharmaceutical production but also to global procurement policies, so that they increase the potential financial return to local African production.
Right now, most COVID-19 vaccines are owned and produced outside of African countries. How do African countries change this? This year, we will be sharing some exciting reports on how African pharmaceutical hubs can be drawn upon to build the continent’s pharmaceutical industry – including exploring the lessons that can be learnt from other countries such as India and China in building their pharmaceutical industries. Watch this space!
This rich and informative data behind this analysis is available below. Have a read, check out the graphics and numbers below, and do let us know what you conclude and what you’d like us to find out next time!
 To find out how Development Reimagined can support you, your organisation or Government to respond to COVID-19 in a sustainable way please email the team at clients@developmentreimagined.com.
To find out how Development Reimagined can support you, your organisation or Government to respond to COVID-19 in a sustainable way please email the team at clients@developmentreimagined.com.
Special thanks go to Rosie Flowers-Wanjie, Osaru Omosigho, David Tinashe Nyagweta and Jing Cai for their work on the graphics and collecting/analysing the underlying data and this accompanying article.
The data was collated primarily from Africa CDC, as well as other sources including: government websites and media reports, the IMF policy tracker; Worldometer and the New York Times Vaccine Tracker. Our methodology is entirely in-house, based on analysis of vaccine, testing, spending, social distancing, income categories and other trends.
If you spot any gaps or have any enquiries, please send your feedback to us at team@developmentreimagined.com, we will aim to respond asap.
March 2022
