In the past year, cholera has returned to the fore as a public health disease of concern, with current outbreaks being battled in 22 countries across three continents, more than half of which are African countries.
What is cholera, and how can it be avoided? Can it be treated?
Cholera is an acute diarrheal infection characterized by watery diarrhea and potentially fatal dehydration. It is caused by ingesting food or water that is contaminated with the bacterium Vibrio cholerae. It has a short incubation period ranging between two hours and five days.
However, it can be avoided or treated.
Avoiding cholera means avoiding poor sanitation and hygiene, and therefore ensuring quality water infrastructure. Avoiding humanitarian crises and conflict is also key, as this complicates their containment.
Treating cholera often involves rehydration and the use of antibiotics, but there is also a vaccine (Oral Cholera Vaccine (OCV)) which is ideally offered as a two-dose therapy, and can help avoid fatalities.
How big is the current outbreak and how many countries are affected?
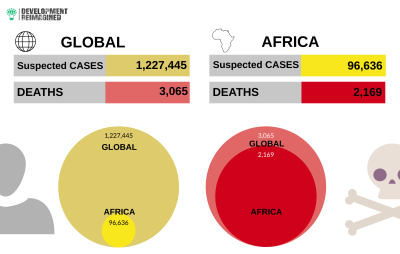
This is one of the largest recorded global cholera outbreaks in decades. As of February 21st 2022, the global total of suspected cases was over 1.22 million with an estimate of 3,065 recorded deaths. However, since most cases are not reported, some studies estimate that typically around 2.9 million cases and 95,000 deaths occur annually.
12 African countries are currently affected: Cameroon, DRC, Ethiopia, Kenya, Malawi, Mozambique, Niger, Nigeria, Somalia, South Sudan, Tanzania, and Zambia. These countries are registering just 7% (96,636) of the global suspected cases but over 70% (2,169) of cholera-related deaths. In other words, this outbreak has a higher case-fatality ratio of 2.04% average in Africa, compared to an estimated 1.45% average globally.
Is there adequate deployment of cholera vaccines in countries that require them?
There are currently seven types of OCVs and primarily manufactured in six countries by six companies: the Republic of Korea (Euvichol by EuBiologics Co.), France (Dukoral by Valneva), China (OraVacs by United Biotech), India (ShanChol by Shantha Biologics, a subsidiary of Sanofi-Pasteur and HillChol by Bharat BioTech), Vietnam (mORCVAX by Vabiotech) and the United States (Vaxchora by Emergent BioSolutions).
But the WHO currently only deems two of the seven vaccines good enough for distribution in its global health programs – ShanChol and Euvichol.
On the African continent, ShanChol is currently manufactured in three countries: Algeria, Egypt, and South Africa. However, a 3-year process is already in train to phase out all of its production in these countries by the end of 2023. On the other hand, additional manufacturing investments in an OCV on the continent is reportedly in train, e.g., by Biovac, a South African based pharmaceutical company, supported by Wellcome and the Bill & Melinda Gates Foundation.
Is it costly to buy these vaccines?
OCVs can cost the same or lower than COVID vaccines. Pre-COVID prices for OCV (plastic packaging) were recorded by UNICEF in 2018 at US$ 1.2–1.3 per single dose, and have since increased post-COVID to US$ 1.1–1.65 per single dose in 2023. Glass-packaged doses went up from US$ 1.85 per single dose in 2018 to US$ 3.13–4 in 2023.
In comparison, the COVID vaccine costs varied between US$ 0.3 – 5.5 for single doses across a selection of manufacturers in 2021/22.
How many vaccines are available, and how many are needed?
Eight of the affected African countries have already launched OCV vaccination campaigns –Cameroon, DRC, Kenya, Niger, Nigeria, Malawi, Mozambique and Somalia. In addition, these affected states are engaging in measures such as establishing task forces to improve OCV spread and acceptance, healthcare staff training, and introducing new water, sanitation and hygiene campaigns and initiatives.
However, current vaccine campaigns require around 1.5 – 2 million doses per country to attempt coverage of the most at-risk populations (90-100% of persons) in hotspots. That would imply for Africa, for example, that at least 18 million doses are required asap, through purchase or distribution through WHO and others.
However, the coverage is highly inconsistent. In 2021, African countries received 15.6 million doses in total; received 16 million doses in 2022; and so far in 2023, Mozambique has received over 719,000 doses and about 4.8 million doses for Malawi.
Part of the reason for the inconsistency is that only 36 million doses were projected to be produced in 2022 globally – this is insufficient. Emergency stockpiles are only growing slowly and are projected at 6 million doses this month – African countries are at the back of the queue. On October 20th, 2022, members of the International Coordinating Group (ICG) – IFRC, MSF, UNICEF, and WHO – took the unprecedented decision to temporarily limit all reactive OCV campaigns to one single dose so that they can spread doses further, even though the protective period will be shorter. This may help but could create more inconsistencies.
What more needs to be done?
Cholera can be contained. But the higher death rate in African countries suggests treatments and vaccines are simply not getting to where they need to. Part of this is due to a lack of production on the continent, plus low levels of global vaccine production.
Addressing this will therefore require additional manufacturing pacts between African states and other OCV brands / manufacturers, such as OraVacs in China; as well the WHO working to swiftly approve more OCV types to improve global supply.
In the long-term however, vaccines are not the panacea. Cholera will only be really addressed by higher and consistent investment in water and other infrastructure in all countries.

March 2023
